



Executive Summary
- Nipah virus is an enveloped, single-stranded RNA virus in the paramyxovirus family and a World Health Organization priority pathogen, with case fatality rates of 40% to 75% in reported outbreaks. It combines zoonotic spillover from fruit bat reservoirs, documented human-to-human transmission, and the absence of approved vaccines or targeted antivirals, placing it among a small group of pathogens with clear epidemic and pandemic potential. The WHO has recently reported confirmed cases in West Bengal, India.
- Clinical disease ranges from mild febrile illness to fatal encephalitis. Patients typically develop fever, headache, muscle pain, and vomiting before progressing to seizures, altered consciousness, and coma. Respiratory symptoms are associated with higher mortality, and some survivors develop delayed or relapsing encephalitis months or years later. Diagnostics rely primarily on RT-PCR and serological assays, with no validated point-of-care tests yet available.
- Research has accelerated sharply since 2018, with patent activity growing nearly fourfold between 2021 and 2025. Therapeutic candidates under investigation include the monoclonal antibody m102.4 in Phase I trials, repurposed antivirals such as remdesivir and favipiravir, and host-targeted approaches. Vaccine candidates in clinical trials include ChAdOx1 NiVB (Phase II), PHV02, and Moderna and NIAID's mRNA-1215, all targeting the viral glycoproteins required for host cell entry.
With the WHO reporting newly confirmed Nipah virus cases in West Bengal, India and Asian countries rushing to tighten airport health screenings, the world is once again on alert for a deadly pathogen. Nipah virus periodically re‑emerges in South and Southeast Asia, and even a handful of cases draw global attention because of the virus’s exceptionally high fatality rate, which can exceed 50% in many outbreaks. The virus combines three high-risk features: zoonotic spillover from wildlife reservoirs, documented human-to-human transmission, and the absence of approved vaccines or targeted antivirals. These characteristics place Nipah virus among a small group of pathogens with clear epidemic and pandemic potential. Its inclusion in the WHO’s R&D Blueprint for priority pathogens reflects the severity of disease and persistent gaps in medical countermeasures.
Virology of Nipah virus: Molecular architecture and host invasion
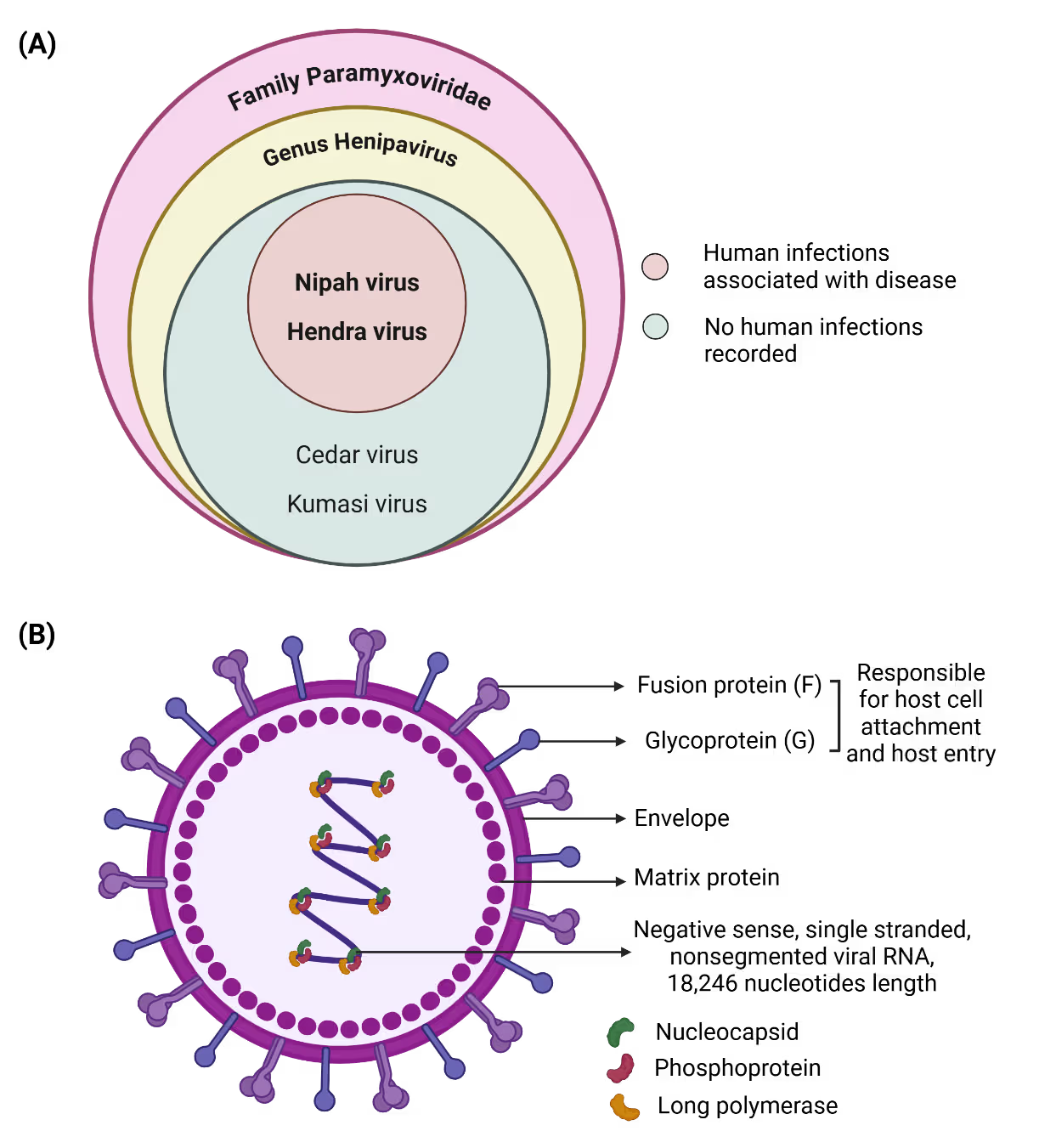
Nipah virus is an enveloped, negative-sense, single-stranded RNA virus with a genome of approximately 18.2 kilobases that belongs to the paramyxoviridae family (Figure 1A). The genome encodes six major structural proteins that coordinate viral replication, assembly, and host cell entry. Among these, the attachment (G) and fusion (F) glycoproteins are central to host tropism and pathogenicity (Figure 1B).
Is your R&D data ready for the future? The CAS Intelligence Hub is a powerful integrated solution that transforms fragmented scientific R&D data into a harmonized, AI-ready knowledge environment.
Nipah virus uses the ephrin‑B2 and ephrin‑B3 receptors, which are widely conserved and expressed in endothelial cells, neurons, and respiratory epithelium, enabling infection across multiple organs and species. After entry, the virus suppresses interferon signaling, allowing rapid replication and causing widespread endothelial injury, vasculitis, and central nervous system inflammation. Evidence of relapsing and late‑onset encephalitis suggests that Nipah can persist in immune‑privileged sites, though the mechanisms of this long‑term persistence remain poorly understood.
Spillover geography and transmission pathways
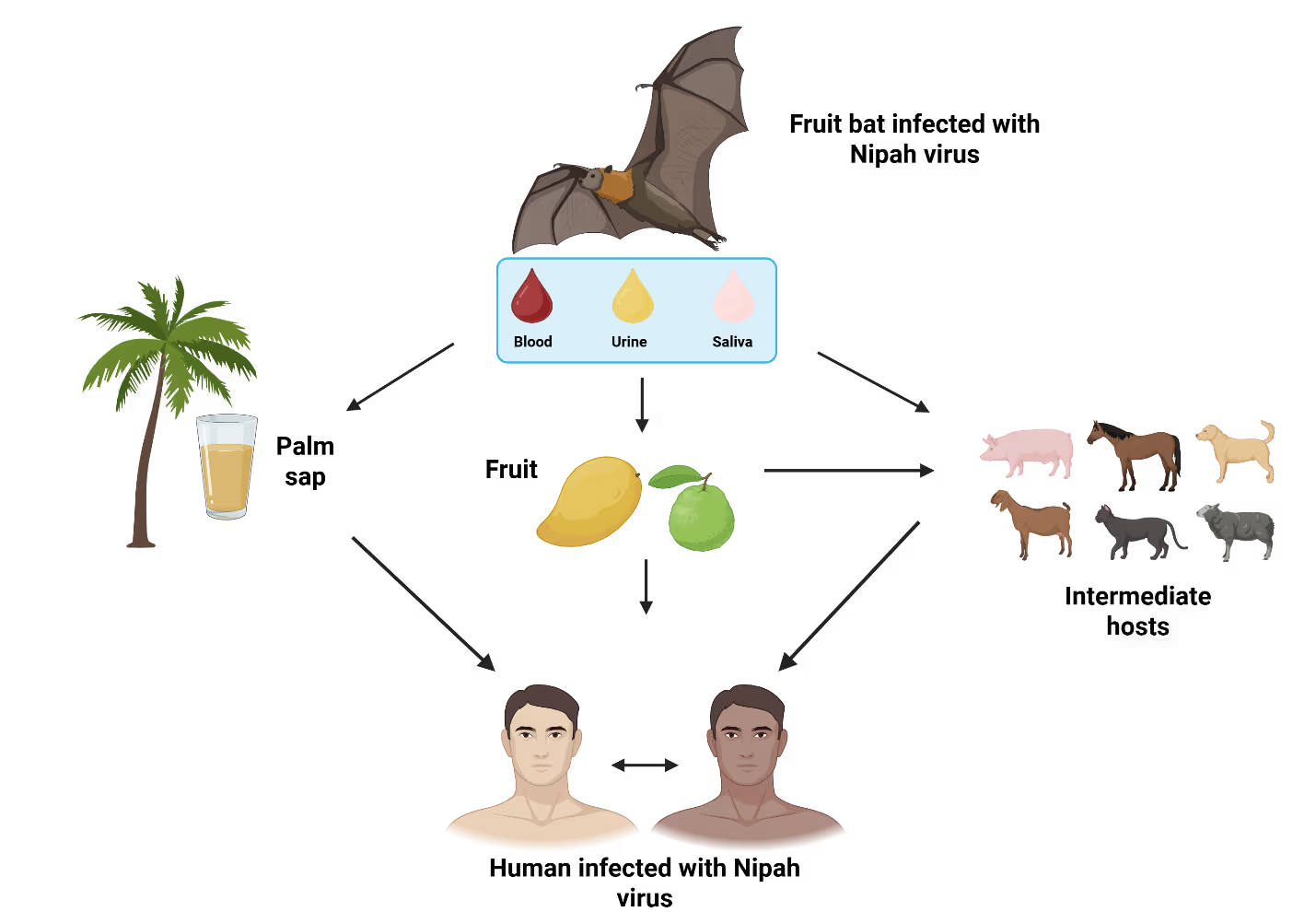
Nipah virus outbreaks have been reported in Malaysia, Singapore, Bangladesh, India, and the Philippines, showing a concentrated yet varied spillover landscape. The first major outbreak occurred in Malaysia (1998–1999), where pigs acted as amplifying hosts and facilitated large-scale animal-to-human transmission, with additional spread to Singapore through imported pigs. Since 2001, Bangladesh has experienced near annual outbreaks primarily linked to consumption of bat-contaminated raw date palm sap and subsequent human-to-human transmission, a pattern also observed in India, especially in West Bengal and Kerala. In the Philippines, outbreaks have involved horse-to-human transmission followed by person-to-person spread. Across affected regions, case fatality rates remain high (40–75%) and often rise during outbreaks dominated by interpersonal transmission. This person‑to‑person spread typically occurs through direct contact with bodily fluids of infected individuals, including saliva, respiratory secretions, blood, and urine, with additional risk from contaminated surfaces and close‑range exposure to respiratory droplets in crowded or poorly ventilated settings. Environmental change and increasing bat-human interface continue to elevate spillover risks, underscoring the need for coordinated One Health surveillance (Figure 2).
Natural reservoirs
Fruit bats of the family Pteropodidae, particularly Pteropus species, are the confirmed natural hosts of Nipah virus. These bats do not develop overt disease but they shed the virus through saliva, urine, and excreta. Viral shedding intensifies in pregnant bats during winter, coinciding with the date palm sap harvesting season in endemic regions. Pteropus bats are widely distributed across South Asia and northern Australia.
Infection in domestic animals
Multiple domestic animals, including pigs, horses, goats, sheep, cats, and dogs, have been infected during past outbreaks, with pigs playing a central role during the 1999 Malaysian epidemic. Infected pigs can shed virus even during the 4-14 day incubation period. Farm-to-farm transmission can occur via contaminated items such as equipment, clothing, boots, or vehicles.
Clinical spectrum of disease: From febrile illness to fatal encephalitis
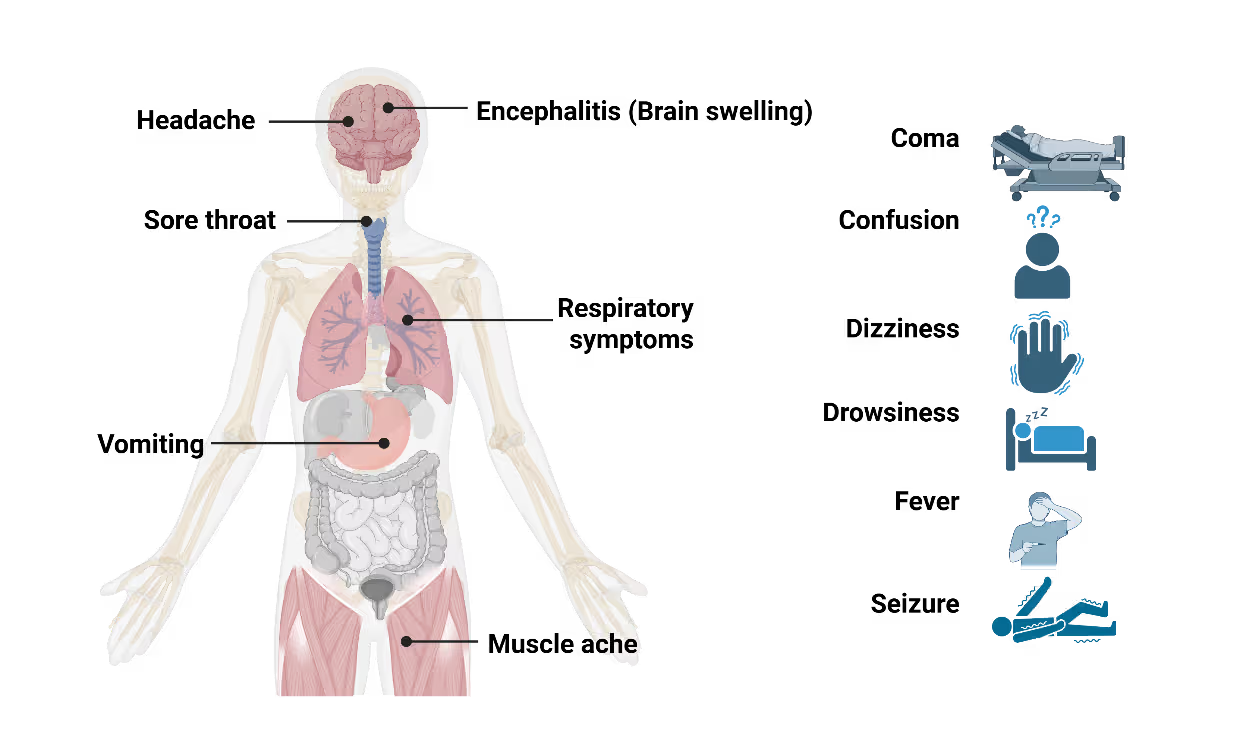
Nipah virus infection presents with a wide clinical spectrum, ranging from mild or asymptomatic cases to rapidly progressive, fatal disease. Initial symptoms are non-specific and include fever, headache, myalgia, and vomiting, making early clinical diagnosis challenging, particularly in resource-limited settings. Neurological involvement is the hallmark of severe disease. Patients may develop acute encephalitis characterized by altered mental status, seizures, and coma within days of symptom onset (Figure 3). Respiratory involvement, including cough and acute respiratory distress, is more frequently observed in outbreaks with sustained human-to-human transmission and is associated with higher mortality. An unusual and clinically significant aspect of Nipah virus infection is the occurrence of delayed or relapsing encephalitis. These cases, reported months or even years after apparent recovery, underscore the need for long-term follow-up of survivors and complicate assessments of disease burden. The incubation period typically ranges from 4 to 14 days but can extend beyond 40 days in rare cases. This prolonged incubation window poses challenges for contact tracing and outbreak containment, particularly during large exposure events.
Research landscape and publication trends
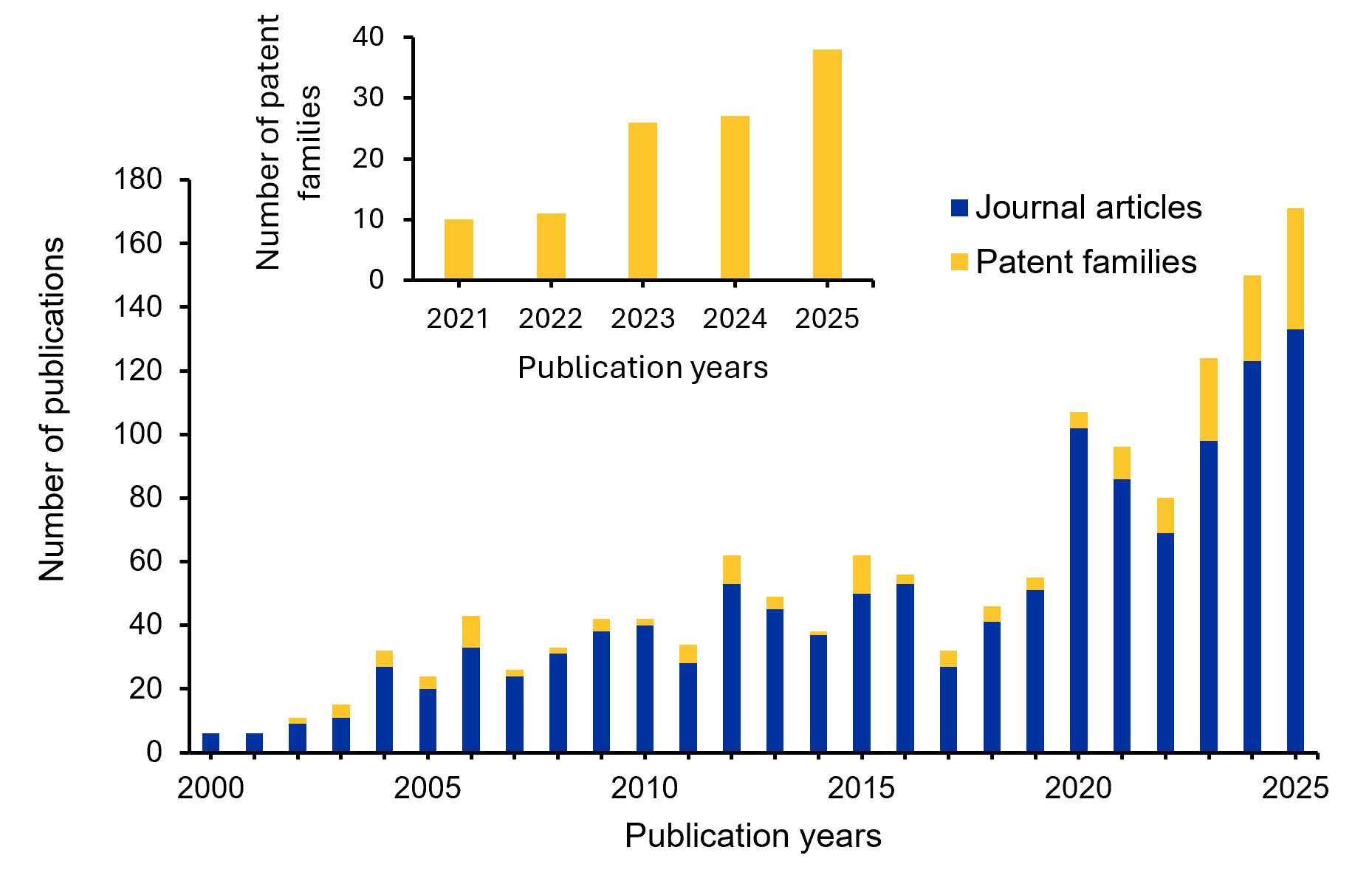
We leveraged the CAS Content Collection™, accessed through CAS IP Finder™ powered by STN™, to analyze global journal publication and patent activity related to Nipah virus. Year-wise trends reveal a steady increase in research output over the past 25 years (Figure 4), with a pronounced rise after 2018 driven by intensified outbreak events and broader recognition of high-risk zoonotic threats. Journal articles remain the dominant form of scholarly output, while patent filings, particularly in the areas of diagnostics, therapeutics, and vaccines, have expanded significantly since 2020. The inset analysis of the last five years shows that patent activity increased from 10 families in 2021 to 38 in 2025, representing an overall 280% growth (~3.8 fold) and a compound annual growth rate of ~39.6%. By 2025, scientific publications and patent activity reach their highest levels, reflecting sustained R&D investment and a strengthened global research focus.
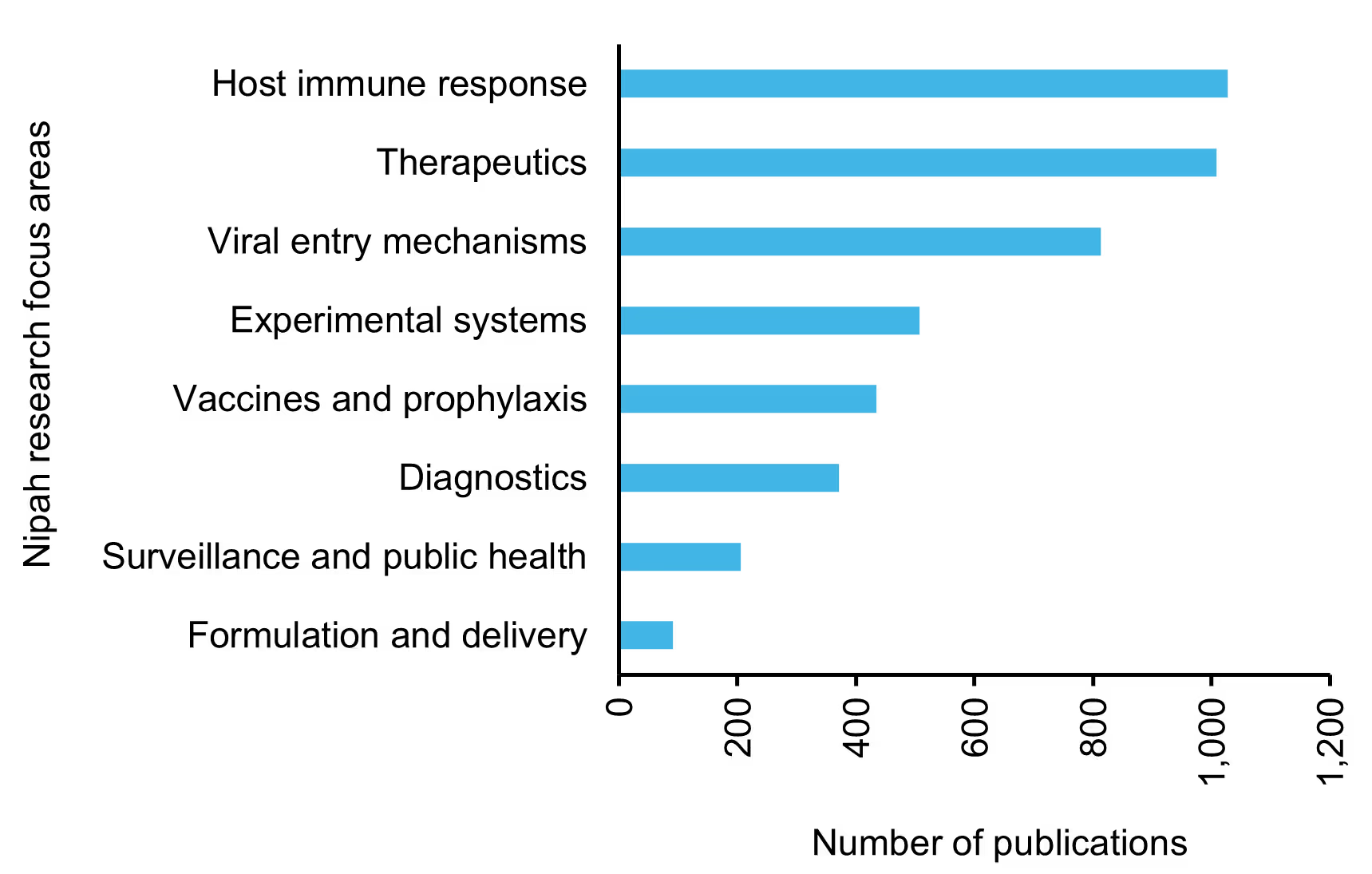
Research is most concentrated in understanding host immune responses, therapeutic development, and viral entry mechanisms, underscoring a strong interest in pathogenesis and intervention strategies. Moderate publication volume is observed in areas such as experimental systems, vaccines, prophylaxis, and diagnostics, whereas surveillance, public health, and formulation and delivery remain relatively underexplored. Together, these insights reveal a research ecosystem driven primarily by mechanistic and therapeutic investigations, with notable gaps in translational readiness and outbreak preparedness.
Using CAS SciFinder® to access the advanced patent‑discovery capabilities of the CAS Content Collection™, we identified a set of recent, high‑relevance patents in Nipah virus R&D. These are summarized in Table 1.
| Patent Number / Year / Title | Key Contribution |
|---|---|
| CN121320643 A / 2026 / RPA-CRISPR/Cas13a-based method and kit for rapid Nipah virus detection | Introduces a rapid, highly sensitive RPA-CRISPR/Cas13a-based Nipah virus detection method capable of delivering results within 35 minutes with a 1 copy/μL detection limit. |
| DE202025104347 U1 / 2025 / A portable device for detecting Nipah virus by means of odor analysis | Introduces a portable AI-enabled volatile organic compounds detection device combining UV-ionization, miniature mass spectrometry, and machine-learning models to identify Nipah virus-specific volatile signatures from air samples. Provides real-time alerts and wireless connectivity for model updates, enabling rapid, contactless screening and early warning of emerging health risks. |
| KR2900650 B1 / 2025 / Immunogenic peptides for Nipah virus vaccine and diagnostic applications | Develops immunogenic peptides based on Nipah virus-specific epitope sequences for use in vaccine formulations and diagnostic applications. |
| CN120420326 A / 2025 / Application of MY-1B in preparing a drug for preventing and treating Nipah virus | Describes a host-directed antiviral strategy by using MY-1B to inhibit host m5C RNA modification by blocking NSUN2 methyltransferase activity, thereby suppressing Nipah virus replication. |
| CN120305267 A / 2025 / Application of STM2457 in preparation of drug for preventing and treating Nipah virus | This approach offers a novel therapeutic strategy by targeting host epigenetic machinery rather than viral components directly. |
| IN202541113726 A / 2025 / De novo multi-epitope immunogen for Nipah virus leveraging reverse vaccinology | Presents a multi-epitope subunit vaccine designed using reverse vaccinology and immunoinformatics, integrating CTL, HTL, and B-cell epitopes from the Nipah virus phosphoprotein with β-defensin as an adjuvant to enhance immune activation. |
| IN202441085121 A / 2024 / Functionalized fullerene conjugated nanomolecules for inhibition of Nipah virus infections | Develops functionalized C20/C60 fullerene nanomolecules that target multiple Nipah virus proteins, disrupting RNA handling, nucleocapsid formation, and virion assembly. This multi-target antiviral mechanism reduces viral propagation and offers potential broad-spectrum activity. |
| WO2024168224 A2 / 2024 / Engineered Nipah virus mRNA vaccine | Describes an mRNA vaccine platform encoding soluble or full-length Nipah virus glycoprotein (NiV-G) and/or fusion protein (NiV-F), designed to elicit a strong immune response against Nipah virus infection. |
| CN117304311A / 2023 / Nanometer antibody and multimerization nanometer antibody targeting Nipah virus G protein | Develops high-affinity nano-antibodies targeting the Nipah virus G protein using a phage-display–derived nano-antibody library. |
| CN110028579 A / 2019 / Monoclonal antibody against envelope glycoprotein and its application in preparation of therapeutic drugs for Nipah virus disease | The monoclonal antibody 14F8 selectively binds the Nipah virus envelope glycoprotein with high affinity while showing minimal crossreactivity to Hendra virus, making it suitable for specific diagnostic applications. |
Patent offices managing examination backlogs or law firms handling complex scientific IP portfolios can explore CAS IP Finder, powered by STN™ capabilities through demonstrations tailored to specific workflow requirements, including chemical structure searching and multi-jurisdiction filing analysis.
Diagnosing a high-consequence pathogen: Tools and limitations
Accurate and timely diagnosis of Nipah virus infection is critical for outbreak control but remains logistically challenging. Due to the non-specific nature of early symptoms, laboratory confirmation is essential. Reverse transcription polymerase chain reaction (RT-PCR) assays are the primary diagnostic tool for detecting viral RNA in acute cases. Serological assays, including enzyme-linked immunosorbent assays (ELISA) for IgM and IgG antibodies, play an important role in retrospective diagnosis and sero-surveillance. Virus isolation and neutralization assays provide definitive confirmation but require biosafety level 4 (BSL-4) containment, severely limiting their accessibility.
In outbreak settings, delays in diagnosis can have significant consequences, allowing continued transmission before infection control measures are implemented. The need for rapid, point-of-care diagnostic tools that can be deployed in decentralized healthcare settings remains a critical unmet need in Nipah virus preparedness.
Therapeutic interventions: Limited options and experimental approaches
Currently, no specific antiviral treatment has been approved for Nipah virus infection, and patient management relies primarily on supportive care. However, ongoing research into antiviral agents, monoclonal antibodies, and host‑targeted therapies continues to expand the landscape of potential interventions.
Recent computational drug‑repurposing studies have highlighted five FDA‑approved antivirals, Saquinavir, Nelfinavir, Simeprevir, Paritaprevir, and Tipranavir, as promising candidates. These compounds demonstrated strong binding affinity to the Nipah virus glycoprotein, host receptor complex, and exhibited stable interactions in molecular docking and molecular dynamics simulations, suggesting their potential for further in vivo and clinical evaluation.
Beyond repurposed antivirals, several experimental molecules, nucleoside analogues, interferon inducers, and monoclonal antibodies have shown varying degrees of efficacy in in vitro, in vivo, or animal model studies. The following table (Table 2) summarizes key drugs and biological therapeutics under investigation for their potential activity against the Nipah virus. Among these, m102.4 is currently in Phase I clinical trials.
| Small molecules | |||
|---|---|---|---|
| Drug | Description | Experimental Model | Mode of action |
| Chloroquine | 4-aminoquinoline (antimalarial) | Syrian golden hamster and ferret | Inhibition of F protein maturation |
| Ribavirin | Guanosine analogue (antiviral) | Open-label clinical trial in humans | Viral replication inhibition |
| Favipiravir | Purine analogue (antiviral) | Syrian golden hamster | Protection against viral challenge |
| Remdesivir (GS-5734) | Adenosine analogue (antiviral) | African green monkey | Nucleotide analogue prodrug; inhibits viral replication |
| Heparin | Anticoagulant | Syrian golden hamster | Inhibits cell-mediated viral trans-infection by binding to heparan sulfate |
| Rintatolimid | Interferon inducer | Syrian golden hamsters | Induces IFN-α and IFN-β production; inhibition of viral replication |
| Griffithsin | Antiviral lectin | Syrian golden hamsters | Inhibits viral entry, replication and syncytia formation |
| VIKI-dPEG4-Toco, VIKI-PEG4-chol | Viral fusion inhibitory peptide | African green monkeys and Syrian golden hamsters | Inhibition of F protein fusion and cell entry |
| Balapiravir (R1479) | Cytidine analogue (antiviral) | In vitro | Viral RNA-dependent RNA polymerase inhibitor |
| Monoclonal antibodies | |||
| Drug | Target | Current stage | Developer |
| mAb 102.4 | NiV G glycoprotein | Human (Phase I trial) ACTRN12615000395538 | Henry M Jackson Foundation for the Advancement of Military Medicine (Bethesda, MD, USA) |
| mAb 5B3, mAb h5B3.1 | NiV pre-fusion F glycoprotein | Preclinical (Mice and ferrets) | University of Washington (Seattle, WA, USA) and Uniformed Services University (Bethesda, MD, USA) |
| mAb HENV-26, mAb HENV-32 | NiV G glycoprotein | Preclinical (Ferrets) | Vanderbilt Vaccine Center (Nashville, TN, USA) |
Vaccine development landscape: Progress amid structural challenges
Nipah virus vaccine development has accelerated in recent years, driven by its designation as a priority pathogen and increased investment from global health preparedness efforts. Multiple platforms, including recombinant subunit vaccines, viral‑vector-based candidates, and nucleic‑acid technologies, are being evaluated across preclinical and early‑phase clinical studies. An overview of the major candidates and their development status is summarized in Table 3-4.
Despite encouraging progress in the laboratory and early clinical evaluations, advancing these candidates toward licensure remains challenging. The sporadic and geographically limited nature of Nipah outbreaks makes traditional efficacy trials difficult to conduct, underscoring the need for alternative regulatory pathways, adaptive trial designs, and region‑specific preparedness strategies.
| Vaccines | Clinical trial phase/Trial ID | Platform | Antigen/immunogen | Sponsor |
|---|---|---|---|---|
| ChAdOx1 NiVB | Phase II | Replication-deficient simian adenoviral vector (ChAdOx1 platform) – same platform as Oxford/AstraZeneca COVID-19 vaccine | Nipah virus glycoprotein (G) encoded in the ChAdOx1 vector | Coalition for Epidemic Preparedness Innovations (CEPI) |
| PHV02 | Phase I / NCT05178901 | Replicating vesicular stomatitis virus (rVSVΔG) viral vector | Expresses recombinant NipahB glycoprotein (NiVG) | Public Health Vaccines LLC |
| mRNA-1215 | Phase I / NCT05398796 (Completed Oct 2025; results posted Oct 23, 2025) | mRNA vaccine in lipid nanoparticles | Prefusion-stabilized F protein covalently linked to G monomer (PreF/G) from NiV-Malaysia strain | National Institute of Allergy and Infectious Diseases (NIAID) and ModernaTX, Inc. |
| Vaccines | Description | Animal Model |
|---|---|---|
| Subunit-based | ||
| HeV-sG (Equivac® HeV) | Subunit vaccine based on soluble HeV G glycoprotein. Elicits cross-protective immune response against HeV and NiV. Available for horses in Australia | Ferret |
| Vector-based | ||
| rVSV-ΔG-NiVB/F-GFP rVSV-ΔG-NiVB/G-GFP |
Recombinant vesicular stomatitis virus (VSV) vaccine expressing NiV-B F or G | African green monkey |
| rRABV/NIV (NIPARAB) | Recombinant rabies virus vector expressing NiV G | C57BL/6 mice |
| rVSV-EBOV-GP-NiV-G | Recombinant VSV vector expressing Ebola virus glycoprotein and NiV G | African green monkey |
| rMV-NiV-G | Recombinant measles virus vaccine (rMV) expressing NiV G | African green monkey |
| BoHV-4-A-CMV-NiV-GΔTK BoHV-4-A-CMV-NiV-FΔTK |
Recombinant bovine herpesvirus vaccine (BoHV) expressing NiV G or NiV F | Pig |
| Virus-like particle-based | ||
| NiV-VLP vaccine | Purified Nipah virus-like particles G, F, and M proteins | Golden Syrian hamster |
| mRNA-based | ||
| sHeVG mRNA LNP | mRNA vaccine encoding soluble HeV glycoprotein (sHeVG) subunit | Syrian hamster |
Conclusion and future outlook
Nipah virus continues to be an emerging pathogen of significant concern. Not only because of its high fatality rate but also due to the complex ecological and molecular factors that sustain its reemergence. As research accelerates across virology, therapeutics, and vaccine development, it is steadily closing knowledge gaps that have long hindered preparedness. Rapid diagnostic advancements, targeted antivirals, and innovative vaccine platforms reflect a broader and more sophisticated R&D ecosystem than at any point since Nipah’s discovery. Yet, the sporadic and geographical nature of outbreaks continues to slow the path from promising laboratory findings to actionable countermeasures. Future progress will depend on strengthening One Health surveillance, improving community‑level early detection, and expanding clinical trial infrastructure in regions where spillover risk is the highest. With sustained investment, cross‑sector collaboration, and adaptive regulatory strategies, the coming decade holds real potential for transformative discoveries. Reducing the global threat of Nipah virus will require scientific innovation but also the long‑term integration of ecological, public health, and clinical insights into cohesive outbreak‑prevention strategies.




