



Executive Summary
- O vírus Ebola pertence à família Filoviridae e existe como múltiplas espécies com patogenicidade variável, com taxas de mortalidade historicamente atingindo 90% em alguns surtos.
- O vírus se espalha através do contato direto com sangue, fluidos corporais e materiais infectados, bem como pela exposição a reservatórios de vida selvagem infectados, como morcegos frugívoros e primatas não humanos.
- A resposta aos surtos evoluiu drasticamente: a epidemia de 2018-2020 na RDC demonstrou o impacto de uma melhor vigilância, diagnósticos rápidos e estratégias de vacinação coordenadas em comparação com epidemias anteriores.
- As vacinas atualmente aprovadas usam plataformas de vetores virais (rVSV e sistemas adenovirais) com eficácia comprovada contra Zaire ebolavirus, mas não existem vacinas licenciadas amplamente distribuídas para as espécies Sudan ou Bundibugyo.
Em maio de 2026, as autoridades de saúde na África Central soaram novamente o alarme sobre um novo surto da doença pelo vírus Ebola (DVE) se espalhando por partes da República Democrática do Congo e Uganda. O que preocupou imediatamente os cientistas foi o envolvimento suspeito da rara cepa Bundibugyo, uma espécie para a qual não existe atualmente nenhuma vacina licenciada validada ou amplamente distribuída. O surto reacendeu rapidamente as discussões sobre a preparação global para surtos, vigilância transfronteiriça, equidade na vacinação e a crescente ameaça de transbordamentos zoonóticos em regiões ecologicamente perturbadas.
Este ressurgimento serve como um lembrete claro de por que o Ebola continua sendo uma das doenças infecciosas mais temidas: as taxas de mortalidade podem chegar a 90%, o vírus se espalha através do contato humano durante os surtos e pode devastar sistemas de saúde já frágeis em poucas semanas. Além das manchetes alarmantes, o Ebola também se tornou um campo de testes crucial para a ciência moderna de surtos, desde a vigilância genômica em tempo real até plataformas de vacinas revolucionárias que foram implantadas em poucos meses durante surtos recentes.
A família do vírus Ebola
O vírus Ebola pertence à família Filoviridae, gênero Orthoebolavirus e é caracterizado por uma estrutura filamentosa e um genoma de RNA de fita simples de sentido negativo (Figura 1). Várias espécies do vírus são conhecidas por infectar humanos, incluindo Zaire ebolavirus (EBOV), vírus do Sudão (SUDV) e vírus Bundibugyo (BDBV), cada um com graus variados de patogenicidade. Entre eles, Zaire ebolavirus tem sido historicamente associado às taxas de mortalidade mais altas, atingindo até 90% em alguns surtos, embora surtos mais recentes com melhor gestão clínica tenham apresentado taxas de letalidade mais baixas. O vírus foi identificado pela primeira vez em 1976 durante surtos simultâneos no que é hoje a República Democrática do Congo e o Sudão, estabelecendo as bases para décadas de investigação virológica e epidemiológica. Compreender essas diferenças entre as espécies é fundamental para a resposta a surtos: cada uma requer abordagens de diagnóstico personalizadas, e a cobertura vacinal varia significativamente; enquanto a Ervebo protege contra Zaire ebolavirus, não existem vacinas licenciadas para as espécies Bundibugyo ou Sudão , deixando as populações vulneráveis durante surtos causados por essas cepas.
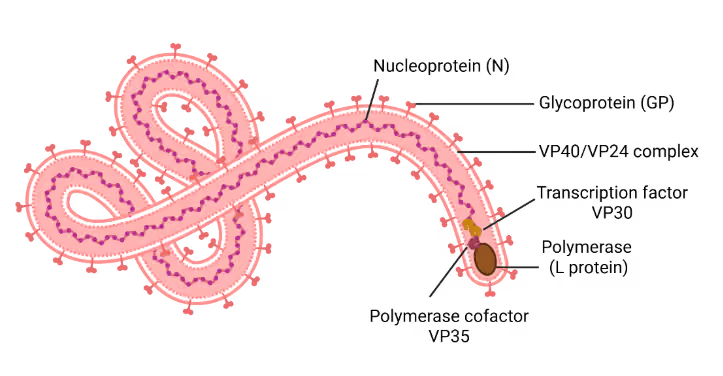
Figura 1: Representação esquemática do vírion do vírus Ebola. Ilustração criada usando BioRender
Manifestação da doença e dinâmica de transmissão
A doença pelo vírus Ebola (EVD) é uma enfermidade aguda, frequentemente grave, caracterizada por sintomas inespecíficos, como febre de início súbito, fadiga, mialgia, dor de cabeça e dor de garganta, que podem evoluir para vômitos, diarreia, erupções cutâneas, comprometimento da função renal e hepática e, em muitos casos, hemorragias internas e externas. A transmissão ocorre por contato direto com sangue, secreções, órgãos ou outros fluidos corporais de indivíduos infectados ou superfícies contaminadas, bem como pela exposição a animais selvagens infectados (particularmente morcegos frugívoros e primatas não humanos), que são considerados reservatórios naturais. A patogênese da EVD envolve a entrada viral através de superfícies mucosas ou pele lesionada, seguida de replicação rápida em monócitos, macrófagos e células dendríticas, levando a respostas imunes desreguladas, tempestade de citocinas e danos teciduais generalizados. Isso é acompanhado por disfunção endotelial, coagulopatia e aumento da permeabilidade vascular, resultando em falência de múltiplos órgãos e, em casos graves, morte.
Principais surtos de Ebola
Vários surtos de Ebola ocorreram desde 1976. A maior e mais devastadora epidemia ocorreu na África Ocidental entre 2014 e 2016, afetando principalmente a Guiné, a Libéria e a Serra Leoa, com mais de 28.600 casos e 11.300 mortes (Figura 2). A escala desta epidemia sobrecarregou sistemas de saúde frágeis, expondo lacunas críticas na preparação, incluindo a escassez de equipamentos de proteção individual, profissionais de saúde treinados e capacidade de diagnóstico, causando medo generalizado e perturbação econômica. Respostas internacionais atrasadas, combinadas com desconfiança social e desinformação, dificultaram ainda mais os esforços de controle.
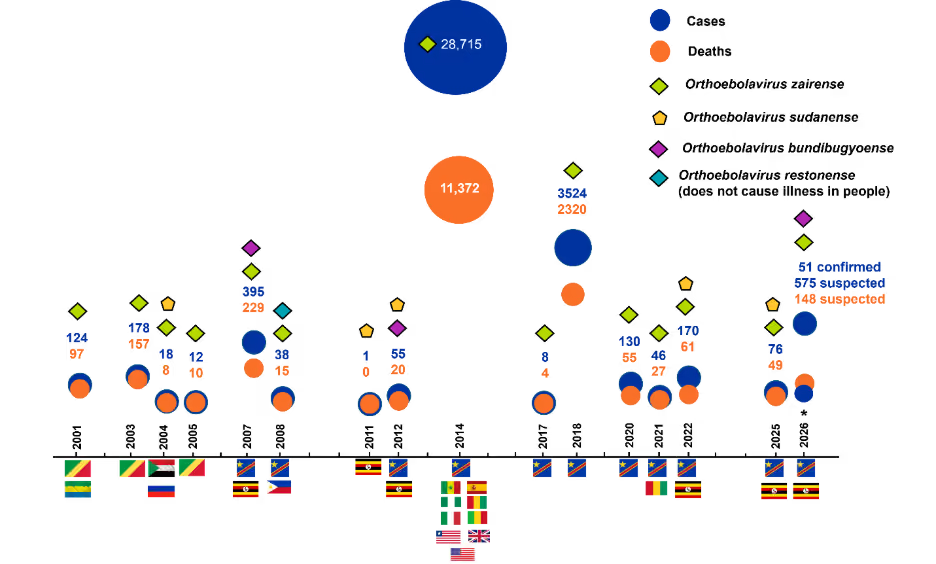
Figura 2: Tendências nos surtos da doença pelo vírus Ebola (2001–2026), mostrando casos e mortes entre países e surtos. Marcadores coloridos denotam espécies de Ebolavirus, destacando padrões na distribuição geográfica e ocorrência específica de cepas. *Dados para 2026 estão incluídos até 21 de maio. Fonte: Centros de Controle e Prevenção de Doenças
Outro grande surto ocorreu na República Democrática do Congo (RDC) entre 2018 e 2020, resultando em aproximadamente 3.481 casos e 2.299 mortes, apesar de desafios como conflitos armados e deslocamento populacional. Crucialmente, este surto demonstrou como é uma preparação eficaz: melhor vigilância, diagnósticos rápidos, estratégias de vacinação e resposta global coordenada contribuíram para uma contenção mais eficaz em comparação com epidemias anteriores.
Zaire ebolavirus tem sido responsável por quase todos os grandes surtos, incluindo a epidemia de 2014–2016, enquanto os vírus Sudão e Bundibugyo causaram surtos menores e geralmente menos frequentes. Em todos os surtos, as taxas de letalidade permanecem altas, geralmente com média em torno de 50% e variando de ~25% a 90%, dependendo do surto e da cepa. Surtos recorrentes e localizados, particularmente na RDC, destacam a natureza endêmica contínua da doença pelo vírus Ebola na África Central.
Tendências globais em pesquisa e inovação sobre o Ebola
Uma análise das tendências de publicações e patentes usando o CAS SciFinder® e CAS IP Finder, com tecnologia STNTM, ferramentas que fornecem acesso à CAS Content Collection™, o maior repositório de informações científicas publicadas com curadoria humana, oferece uma visão geral da atividade de pesquisa relacionada ao Ebolavirus ao longo do tempo (Figura 3). A pesquisa sobre o Ebola tem sido predominantemente impulsionada pela produção acadêmica, com publicações em periódicos representando a maioria (~63%) e superando substancialmente a atividade de patentes. Essa distribuição indica uma forte ênfase na ciência fundamental e exploratória, em vez da comercialização imediata. No entanto, o aumento paralelo nos pedidos de patentes, juntamente com as publicações, reflete uma mudança gradual em direção à pesquisa aplicada e ao desenvolvimento terapêutico à medida que observamos mais surtos.
Os dados revelam um padrão preocupante: esperamos por desastres para agir. A atividade de pesquisa aumenta drasticamente após grandes surtos e, em seguida, estabiliza. Esse ciclo reativo nos deixa perpetuamente despreparados. A epidemia de 2014–2016, por si só, catalisou avanços sem precedentes no desenvolvimento de vacinas e medicamentos baseados em anticorpos, demonstrando tanto a capacidade da sociedade para a inovação rápida quanto a tendência de se desengajar assim que as manchetes desaparecem. Isso levanta uma questão crítica: como podemos sustentar o impulso da pesquisa entre os surtos para garantir uma preparação genuína?
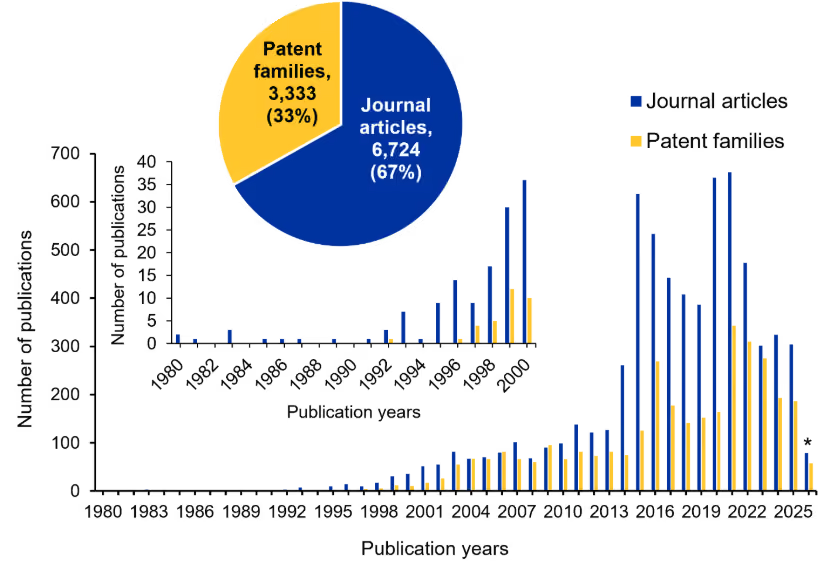
Figura 3 Tendências anuais na produção de pesquisa sobre Ebola, mostrando artigos de periódicos e famílias de patentes de 1980 a 2026. O detalhe destaca a atividade inicial (1980–2000), e o gráfico de pizza resume a distribuição geral de artigos de periódicos e famílias de patentes. *Os dados de 2026 são parciais até 21 de maio. Fonte: CAS Content Collection.
Cenário de ensaios clínicos da doença pelo vírus Ebola
Os dados de ensaios clínicos para a doença pelo vírus Ebola refletem mudanças nas prioridades de pesquisa e um pipeline de desenvolvimento em amadurecimento. Os ensaios concluídos estão concentrados em grande parte nas fases iniciais, enquanto os estudos em andamento estão principalmente nas Fases II–III e Fase IV, indicando a progressão de candidatos existentes em vez da expansão de novos. O número limitado de ensaios ativos de Fase I sugere uma desaceleração na inovação em estágio inicial (Figura 4A).
Estudos focados em vacinas dominam os ensaios concluídos e em andamento, com comparativamente menos investigações terapêuticas (Figura 4B; veja a Tabela 1 para mais detalhes sobre o desenvolvimento de vacinas). Esse desequilíbrio reflete os desafios inerentes à pesquisa sobre Ebola, incluindo a viabilidade de ensaios dependentes de surtos, requisitos rigorosos de biossegurança e restrições logísticas.
Obstáculos operacionais também moldaram o cenário dos ensaios. A realização de estudos durante surtos levanta desafios éticos e práticos, como definir grupos de controle, obter consentimento informado em condições de crise e manter a infraestrutura em regiões com recursos limitados ou afetadas por conflitos. Requisitos de cadeia de frio, escalabilidade de fabricação e desconfiança da comunidade complicam ainda mais a execução.
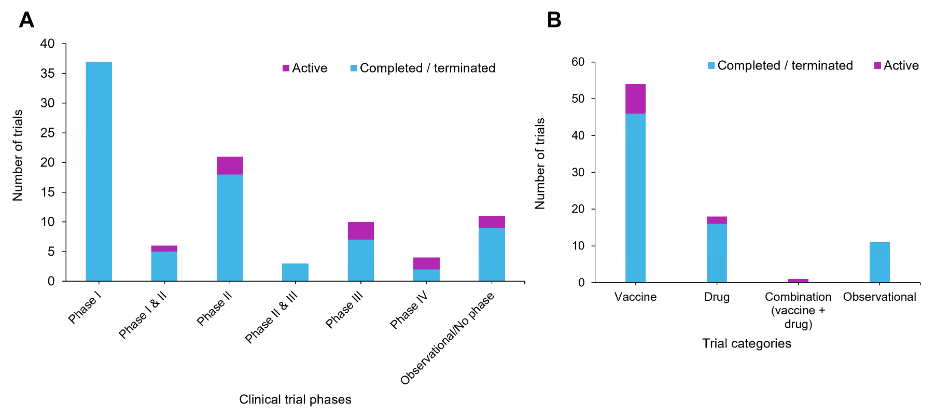
Figura 4: Distribuição de ensaios clínicos de intervenções para a doença pelo vírus Ebola. (A) Distribuição por fase dos ensaios clínicos categorizados como concluídos e em andamento em diferentes fases de estudo. (B) Distribuição dos ensaios clínicos por tipo de intervenção para estudos concluídos e em andamento. Fonte: ClinicalTrials.gov acessado em 21 de maio de 2026
Apesar dessas barreiras, a pesquisa sobre o Ebola impulsionou inovações importantes. Projetos de ensaios adaptativos, vias regulatórias rápidas e modelos de engajamento da comunidade surgiram para equilibrar a urgência com a segurança. Notavelmente, os ensaios de vacinação em anel forneceram uma abordagem ética e eficiente para avaliar vacinas. Essas inovações informaram posteriormente as estratégias clínicas e regulatórias da COVID-19, ressaltando o impacto mais amplo do Ebola na preparação para epidemias.
Terapêutica para Ebola: Status atual e desafios
O desenvolvimento terapêutico para a EVD tem se concentrado em agentes antivirais e intervenções baseadas em anticorpos monoclonais, sendo que estes últimos demonstraram o sucesso clínico mais significativo. Terapias com anticorpos monoclonais, como Inmazeb (REGN-EB3) e ansuvimab (Ebanga), mostraram reduções substanciais na mortalidade em ensaios clínicos randomizados e receberam aprovação da FDA em 2020. Essas terapias atuam visando a glicoproteína viral, neutralizando assim a entrada do vírus e promovendo a eliminação viral.
Em contraste, antivirais de moléculas pequenas que visam a RNA polimerase viral, incluindo o remdesivir, demonstraram eficácia comparativamente limitada em ambientes clínicos. Outras abordagens investigacionais, como favipiravir, galidesivir, e brincidofovir, mostraram resultados promissores in vitro ou em estágios pré-clínicos iniciais, mas produziram resultados inconsistentes ou inconclusivos na avaliação clínica. Terapias baseadas em interferência de RNA, incluindo formulações de siRNA como o TKM-130803, também foram exploradas, embora os benefícios clínicos permaneçam não comprovados. Apesar desses avanços, o pipeline terapêutico permanece relativamente restrito, com poucos candidatos novos progredindo no desenvolvimento em estágio inicial. Desafios persistentes, incluindo a execução de ensaios dependentes de surtos, altos requisitos de biossegurança e limitações de infraestrutura, continuam a restringir a expansão e a diversificação das estratégias terapêuticas nesta área.
Vacinas contra o Ebola: Progresso e direções futuras
O desenvolvimento da vacina contra o Ebola progrediu de conceitos experimentais para estratégias preventivas validadas, com múltiplas vacinas agora aprovadas para uso. Plataformas baseadas em vetores virais, particularmente o vírus da estomatite vesicular recombinante (rVSV) e sistemas adenovirais, dominam o cenário atual, refletindo a convergência em torno de tecnologias eficazes e escaláveis. Essas vacinas diferem em seu design, oferecendo compensações entre proteção rápida de dose única, adequada para o controle de surtos, e regimes de múltiplas doses que proporcionam uma imunidade mais ampla e potencialmente mais duradoura. Apesar do sucesso demonstrado, permanecem desafios importantes, incluindo requisitos de cadeia de frio, conformidade com múltiplas doses e a influência da imunidade pré-existente ao vetor. As principais características das vacinas atualmente aprovadas estão resumidas na Tabela 1. Consequentemente, os esforços atuais são direcionados para abordagens de próxima geração que priorizam a preparação proativa, incluindo cobertura contra pan-filovírus, melhor termoestabilidade, imunidade de maior duração e plataformas adaptáveis, como o mRNA. Essa mudança sinaliza uma transição da resposta reativa a surtos para a prontidão estratégica, apoiada por avanços na fabricação, armazenamento e capacidades de implantação rápida.
Tabela 1: Principais características das vacinas aprovadas contra o Ebola
Como podemos prevenir futuros surtos da doença pelo vírus Ebola?
O contraste entre os surtos de 2014–2016 e 2018–2020 ilustra o que uma preparação eficaz pode alcançar: a implantação precoce de vacinas, o melhor envolvimento da comunidade e uma resposta internacional coordenada reduziram significativamente a mortalidade. No entanto, lacunas críticas permanecem. Ainda carecemos de vacinas amplamente validadas e implantáveis para espécies nãoZaire Ebolavirus , as opções terapêuticas permanecem limitadas e caras, e o financiamento da pesquisa continua seu ciclo de altos e baixos atrelado à ocorrência de surtos, em vez de uma preparação sustentada.
Talvez o mais importante, a prevenção de surtos por meio de abordagens de Saúde Única, incluindo a redução do desmatamento, a melhoria das práticas de manuseio de carne de caça e o fortalecimento da vigilância de doenças em animais selvagens, recebe muito menos atenção do que a resposta a surtos. Como o ressurgimento de espécies raras, como Bundibugyo , destaca, a dependência de estratégias reativas representa riscos contínuos. O investimento sustentado, o acesso equitativo a contramedidas médicas e a integração de perspectivas ecológicas na prevenção de doenças devem se tornar a norma, não a exceção.




