



Executive Summary
- Ebola virus belongs to the Filoviridae family and exists as multiple species with varying pathogenicity, with mortality rates historically reaching 90% in some outbreaks.
- The virus spreads through direct contact with blood, bodily fluids, and infected materials, as well as exposure to infected wildlife reservoirs such as fruit bats and nonhuman primates.
- Outbreak response has evolved dramatically: the 2018-2020 DRC epidemic demonstrated the impact of improved surveillance, rapid diagnostics, and coordinated vaccination strategies compared to earlier epidemics.
- Currently approved vaccines use viral vector platforms (rVSV and adenoviral systems) with proven efficacy against Zaire ebolavirus, but no widely deployed licensed vaccines exist for Sudan or Bundibugyo species.
In May 2026, health authorities in Central Africa once again sounded the alarm over a new outbreak of Ebola virus disease (EVD) spreading across parts of the Democratic Republic of Congo and Uganda. What immediately concerned scientists was the suspected involvement of the rare Bundibugyo strain, a species for which no specifically validated or widely deployed licensed vaccine currently exists. The outbreak rapidly reignited discussions around global outbreak preparedness, cross-border surveillance, vaccine equity, and the growing threat of zoonotic spillovers in ecologically disrupted regions.
This renewed emergence serves as a stark reminder of why Ebola remains one of the most feared infectious diseases: mortality rates can reach 90%, the virus spreads through human-to-human contact during outbreaks, and it can devastate already fragile healthcare systems within weeks. Beyond the alarming headlines, Ebola has also become a crucial testing ground for modern outbreak science, from real-time genomic surveillance to revolutionary vaccine platforms that were deployed within months during recent outbreaks.
The Ebola virus family
Ebola virus belongs to the family Filoviridae, genus Orthoebolavirus and is characterized by a filamentous structure and a negative-sense single-stranded RNA genome (Figure 1). Several species of the virus are known to infect humans, including Zaire ebolavirus (EBOV), Sudan virus (SUDV), and Bundibugyo virus (BDBV), each with varying degrees of pathogenicity. Among these, Zaire ebolavirus has historically been associated with the highest mortality rates, reaching up to 90% in some outbreaks, although more recent outbreaks with improved clinical management have shown lower case fatality rates. The virus was first identified in 1976 during simultaneous outbreaks in what is now the Democratic Republic of the Congo and Sudan, laying the foundation for decades of virological and epidemiological investigation. Understanding these species differences is critical for outbreak response: each requires tailored diagnostic approaches, and vaccine coverage varies significantly, while Ervebo protects against Zaire ebolavirus, no licensed vaccines exist for Bundibugyo or Sudan species, leaving populations vulnerable during outbreaks caused by these strains.
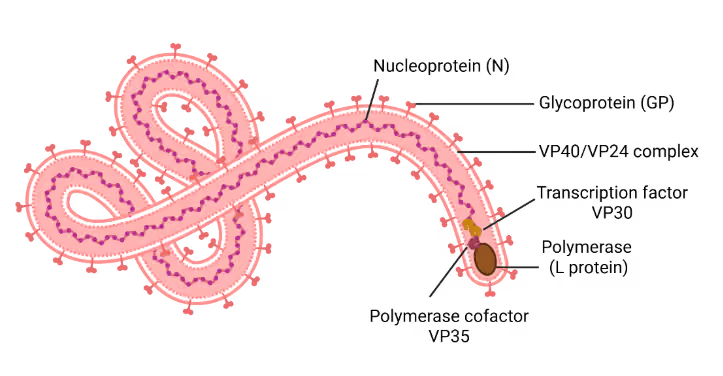
Figure 1: Schematic representation of the Ebola virus virion. Illustration created using BioRender
Disease manifestation and transmission dynamics
Ebola virus disease (EVD) is an acute, often severe illness characterized by nonspecific symptoms such as sudden-onset fever, fatigue, myalgia, headache, and sore throat, which can progress to vomiting, diarrhea, rash, impaired kidney and liver function, and, in many cases, internal and external hemorrhaging. Transmission occurs through direct contact with blood, secretions, organs, or other bodily fluids of infected individuals or contaminated surfaces, as well as through exposure to infected wildlife (particularly fruit bats and nonhuman primates), which are considered natural reservoirs. The pathogenesis of EVD involves viral entry via mucosal surfaces or broken skin, followed by rapid replication in monocytes, macrophages, and dendritic cells, leading to dysregulated immune responses, cytokine storm, and widespread tissue damage. This is accompanied by endothelial dysfunction, coagulopathy, and increased vascular permeability, resulting in multiorgan failure and, in severe cases, death.
Major Ebola outbreaks
Several Ebola outbreaks have occurred since 1976. The largest and most devastating epidemic occurred in West Africa between 2014 and 2016, primarily affecting Guinea, Liberia, and Sierra Leone, with over 28,600 cases and 11,300 deaths (Figure 2). The scale of this epidemic overwhelmed fragile healthcare systems, exposing critical gaps in preparedness, including shortages of personal protective equipment, trained healthcare workers, and diagnostic capacity, causing widespread fear and economic disruption. Delayed international responses, combined with social mistrust and misinformation, further hindered control efforts.
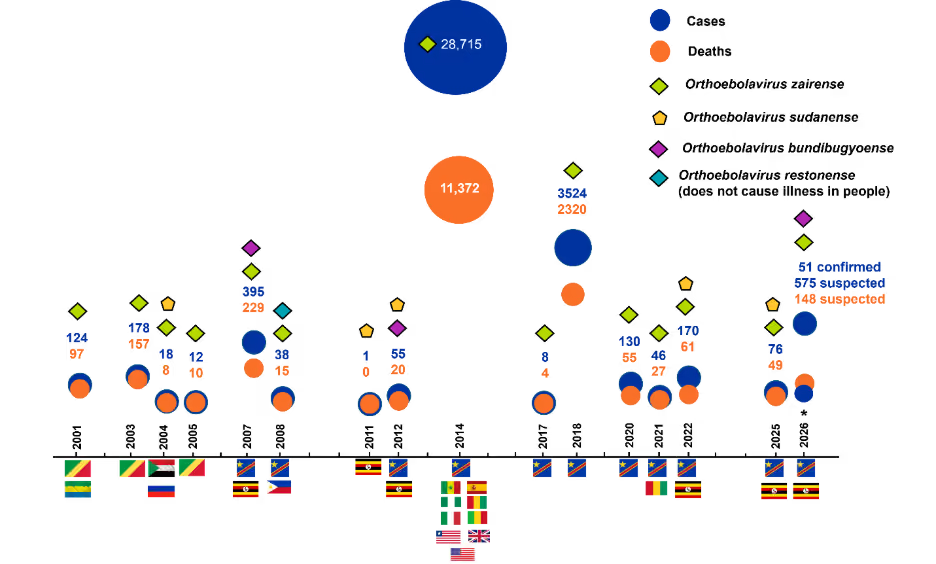
Figure 2: Trends in Ebola virus disease outbreaks (2001–2026), showing cases and deaths across countries and outbreaks. Colored markers denote Ebolavirus species, highlighting patterns in geographic distribution and strain-specific occurrence. *Data for 2026 are included up to May 21. Source: Centers for Disease Control and Prevention
Another major outbreak occurred in the Democratic Republic of Congo (DRC) between 2018 and 2020, resulting in approximately 3,481 cases and 2,299 deaths despite challenges such as armed conflict and population displacement. Crucially, this outbreak demonstrated what effective preparedness looks like: improved surveillance, rapid diagnostics, vaccination strategies, and coordinated global response contributed to more effective containment compared to earlier epidemics.
Zaire ebolavirus has been responsible for nearly all large outbreaks, including the 2014–2016 epidemic, whereas Sudan and Bundibugyo viruses have caused fewer and generally smaller outbreaks. Across outbreaks, case fatality rates remain high, typically averaging around 50% and ranging from ~25% to 90% depending on the outbreak and strain. Recurring, localized outbreaks, particularly in the DRC, highlight the continued endemic nature of Ebola virus disease in Central Africa.
Global trends in Ebola research and innovation
An analysis of publication and patent trends using CAS SciFinder® and CAS IP Finder, powered by STNTM, tools that provide access to the CAS Content Collection™, the largest human-curated repository of published scientific information, offers an overview of research activity related to Ebolavirus over time (Figure 3). Ebola research has been predominantly driven by academic output, with journal publications accounting for the majority (~63%) and substantially exceeding patent activity. This distribution indicates a strong emphasis on foundational and exploratory science rather than immediate commercialization. However, the parallel increase in patent filings alongside publications reflects a gradual shift toward applied research and therapeutic development as we see more outbreaks.
The data reveal a troubling pattern: we wait for disasters to act. Research activity surges dramatically after major outbreaks, then plateaus. This reactive cycle leaves us perpetually underprepared. The 2014–2016 epidemic alone catalyzed unprecedented advances in vaccine development and antibody-based therapeutics, demonstrating both society’s capacity for rapid innovation and tendency to disengage once headlines fade. This raises a critical question: How can we sustain research momentum between outbreaks to ensure genuine preparedness?
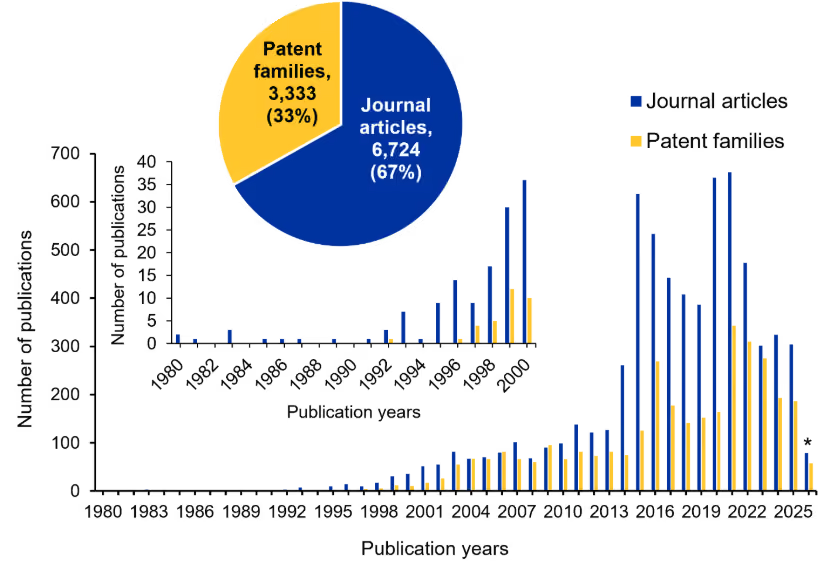
Figure 3 Annual trends in Ebola research output showing journal articles and patent families from 1980-2026. The inset highlights early activity (1980–2000), and the pie chart summarizes the overall distribution of journal articles and patent families. *Data for 2026 is partial through 21 May. Source CAS Content Collection.
Clinical trial landscape of Ebola virus disease
Clinical trial data for Ebola virus disease reflect shifting research priorities and a maturing development pipeline. Completed trials are largely concentrated in early phases, while ongoing studies are primarily in Phase II–III and Phase IV, indicating progression of existing candidates rather than expansion of new ones. The limited number of active Phase I trials suggests a slowdown in early-stage innovation (Figure 4A).
Vaccine-focused studies dominate completed and ongoing trials, with comparatively fewer therapeutic investigations (Figure 4B; see Table 1 for more details on vaccine development). This imbalance reflects inherent challenges of Ebola research, including outbreak-dependent trial feasibility, stringent biosafety requirements, and logistical constraints.
Operational hurdles have also shaped the trial landscape. Conducting studies during outbreaks raises ethical and practical challenges, such as defining control arms, obtaining informed consent in crisis conditions, and maintaining infrastructure in resource-limited or conflict-affected regions. Cold-chain requirements, manufacturing scalability, and community mistrust further complicate execution.
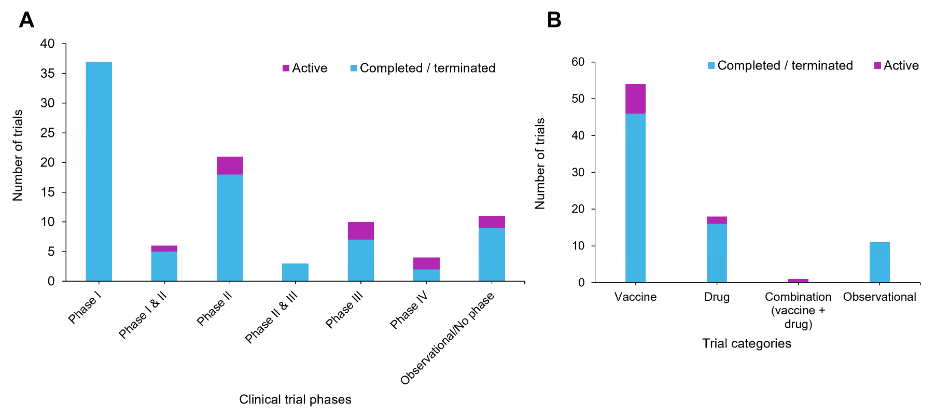
Figure 4: Clinical trial distribution of Ebola virus disease interventions. (A) Phase-wise distribution of clinical trials categorized as completed and ongoing across different trial phases. (B) Distribution of clinical trials by intervention type for both completed and ongoing studies. Source: ClinicalTrials.gov accessed on 21 May 2026
Despite these barriers, Ebola research has driven important innovations. Adaptive trial designs, rapid regulatory pathways, and community engagement models emerged to balance urgency with safety. Notably, ring vaccination trials provided an ethical and efficient approach to evaluating vaccines. These innovations later informed COVID-19 clinical and regulatory strategies, underscoring Ebola’s broader impact on epidemic preparedness.
Ebola therapeutics: Current status and challenges
Therapeutic development for EVD has focused on antiviral agents and monoclonal antibody–based interventions, with the latter demonstrating the most significant clinical success. Monoclonal antibody therapies such as Inmazeb (REGN-EB3) and ansuvimab (Ebanga) have shown substantial reductions in mortality in randomized clinical trials and received FDA approval in 2020. These therapies act by targeting the viral glycoprotein, thereby neutralizing viral entry and promoting viral clearance.
In contrast, small-molecule antivirals targeting viral RNA polymerase, including remdesivir, have demonstrated comparatively limited efficacy in clinical settings. Other investigational approaches, such as favipiravir, galidesivir, and brincidofovir, have shown in vitro or early preclinical promise but yielded inconsistent or inconclusive results in clinical evaluation. RNA interference-based therapies, including siRNA formulations such as TKM-130803, have also been explored, though clinical benefits remain unproven. Despite these advances, the therapeutic pipeline remains relatively narrow, with few novel candidates progressing through early-stage development. Persistent challenges, including outbreak-dependent trial execution, high biosafety requirements, and infrastructural limitations, continue to constrain the expansion and diversification of therapeutic strategies in this area.
Ebola vaccines: Progress and future directions
Ebola vaccine development has progressed from experimental concepts to validated preventive strategies, with multiple vaccines now approved for use. Viral vector–based platforms, particularly recombinant vesicular stomatitis virus (rVSV) and adenoviral systems, dominate the current landscape, reflecting convergence around effective and scalable technologies. These vaccines differ in their design, offering trade-offs between rapid, single-dose protection suitable for outbreak control and multi-dose regimens that provide broader and potentially more durable immunity. Despite demonstrated success, important challenges remain, including cold-chain requirements, multi-dose compliance, and the influence of preexisting vector immunity. Key characteristics of the currently approved vaccines are summarized in Table 1. Consequently, current efforts are directed toward next-generation approaches that prioritize proactive preparedness, including pan-filovirus coverage, improved thermostability, longer-lasting immunity, and adaptable platforms such as mRNA. This shift signals a transition from reactive outbreak response to strategic readiness, supported by advances in manufacturing, stockpiling, and rapid deployment capabilities.
Table 1: Key characteristics of approved Ebola vaccines
How do we prevent future Ebola virus disease outbreaks?
The contrast between the 2014–2016 and 2018–2020 outbreaks illustrates what effective preparedness can achieve: early deployment of vaccines, improved community engagement, and coordinated international response significantly reduced mortality. However, critical gaps remain. We still lack widely validated and deployable vaccines for non-Zaire Ebolavirus species, therapeutic options remain limited and expensive, and research funding continues its boom-bust cycle tied to outbreak occurrence rather than sustained preparedness.
Perhaps most importantly, outbreak prevention through One Health approaches, including reducing deforestation, improving bushmeat handling practices, and strengthening wildlife disease surveillance, receives far less attention than outbreak response. As the re-emergence of rare species such as Bundibugyo highlights, reliance on reactive strategies poses ongoing risks. Sustained investment, equitable access to medical countermeasures, and integration of ecological perspectives into disease prevention must become the norm, not the exception.




